Effects of State Opioid Prescribing Laws on Use of Opioid and Other Pain Treatments Among Commercially Insured U.S. Adults
Abstract
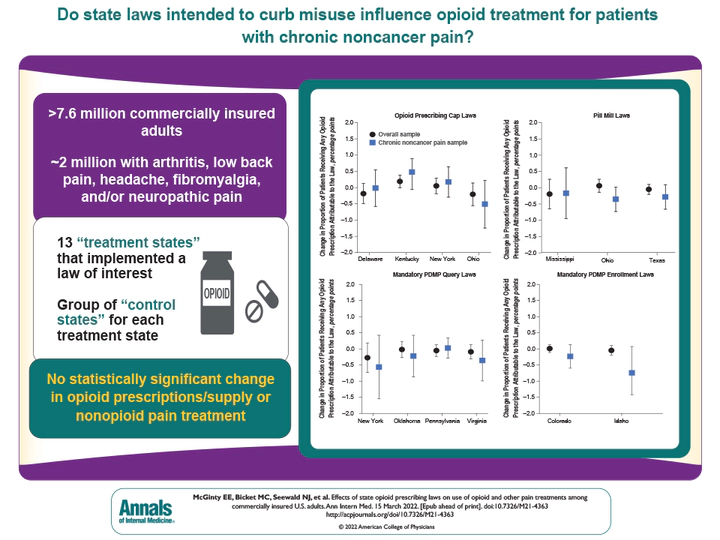
Background: There is concern that state laws to curb opioid prescribing may adversely affect patients with chronic noncancer pain, but the laws’ effects are unclear because of challenges in disentangling multiple laws implemented around the same time.
Objective: To study the association between state opioid prescribing cap laws, pill mill laws, and mandatory prescription drug monitoring program query or enrollment laws and trends in opioid and guideline-concordant nonopioid pain treatment among commercially insured adults, including a subgroup with chronic noncancer pain conditions.
Design: Thirteen treatment states that implemented a single law of interest in a 4-year period and unique groups of control states for each treatment state were identified. Augmented synthetic control analyses were used to estimate the association between each state law and outcomes.
Setting: United States, 2008 to 2019.
Patients: 7 694 514 commercially insured adults aged 18 years or older, including 1 976 355 diagnosed with arthritis, low back pain, headache, fibromyalgia, and/or neuropathic pain.
Measurements: Proportion of patients receiving any opioid prescription or guideline-concordant nonopioid pain treatment per month, and mean days’ supply and morphine milligram equivalents (MME) of prescribed opioids per day, per patient, per month.
Results: Laws were associated with small-in-magnitude and non–statistically significant changes in outcomes, although CIs around some estimates were wide. For adults overall and those with chronic noncancer pain, the 13 state laws were each associated with a change of less than 1 percentage point in the proportion of patients receiving any opioid prescription and a change of less than 2 percentage points in the proportion receiving any guideline-concordant nonopioid treatment, per month. The laws were associated with a change of less than 1 in days’ supply of opioid prescriptions and a change of less than 4 in average monthly MME per day per patient prescribed opioids.
Limitations: Results may not be generalizable to non–commercially insured populations and were imprecise for some estimates. Use of claims data precluded assessment of the clinical appropriateness of pain treatments.
Conclusion: This study did not identify changes in opioid prescribing or nonopioid pain treatment attributable to state laws.
Primary Funding Source: National Institute on Drug Abuse.
Nicholas J. Seewald
Assistant Professor of Biostatistics
Assistant Professor of Biostatistics at the University of Pennsyvlania Perelman School of Medicine